
What is Dissociative Identity Disorder?
Dissociative identity disorder (DID) develops when a person fails to form a total personality that integrates all aspects of yourself or your emotions. To get something labelled as DID, the person must have 2 or more different personality states or alters or identities that control your behaviour at different times. There will be gaps in memories as personalities switch.

Dissociation – Disconnection or disintegration of what are normally psychologically integrated functions. The person may disconnect from their emotions, they won’t feel anything even though they would normally feel terrified. They disconnect from their body, they may not feel as much pain.
In case of trauma, physically or emotionally painful or both if a child or an adult disconnects from themselves, their body, their emotions, their memory, it would help them somewhat to hold the pain. It doesn’t mean that the trauma isn’t traumatic because it still is but overtime when this happens repeatedly they learn more repeatedly to disconnect from themselves so that those traumatic events are not integrated into normal memory and they won’t even recall it. More like a defensive mechanism of the body.
A person without DID sees themselves as being 1 person with different aspects of their personality. A person with DID doesn’t take ownership of the facets. The facets become their own entities with no connection between them. They experience life independent of each other and there may be very little memory shared between them. In DID, people can have gaps in their memory where they can’t account for chunks of time. Say for example you can’t remember driving to a place.
How do people with DID describe their experience?
- When a person who actually has DID walks in for treatment they tend to come in with reports of severe crushing depression that hasn’t responded to any medications or previous trails of psychotherapy.
- In many cases they experience post traumatic stress disorder (PTSD).
- Substance abuse, eating disorder, sleeping troubles.
- Every so often there are people who come in and they are aware or they think they are aware of having dissociative states. This is also not so common.
- They are more embarrassed about their mood changes. Imagine somebody calls us while walking down the street and we certainly don’t have any idea about them. It is mortifying.
- Gaps in memory.
- Watching themselves from outside.
Causes of DID
This mostly happens at childhood but it can develop at any point of life.
- Long term childhood abuse (physical, sexual or emotional) is the most common (90%) one.
- Neglect
- Going through stressful or frightening situation at a young age not knowing what to do.
Tests Done
There are a number of self-report questionnaires which are validated scientifically that can be used. Evidence based interviews, clinical interviews structured for dissociative disorders. Clinicians can use these tools to make an accurate diagnosis. It can also be diagnosed without any tools but the chances of misdiagnosing it is higher.
Brain of People with DID
Brain network patterns distinguish people who are highly dissociative from those who have simple PTSD. In patients with DID, when they are read their trauma stories while they are in the brain scanners so they are essentially having a flashback (they are warned about this). In the brain scanners we can see that some areas of the
- Brain start shutting down
- Less connectivity
- Less brain flow
- Different patterns of neural activation
- Different blood patterns.
- Emotional aroused, jacked up flooded state or the shutdown state.
- Going back and forth between these states.
- Changes in the shape of brain
Researchers not all but some of them have brought professional actors to imitate the brain scans and they can’t do it.
Treatment
Long term trauma based treatment. Treatment is done in stages.
Stage I
As mentioned earlier when the patient comes in they would be struggling with profound depression. Many of them would also have self-harm like cutting or burning. Researchers have claimed that they are some of the most suicidal patients. A lot of stabilisation must be done. They would have problems with sleep. If you don’t get proper sleep you don’t do well. In most cases, nights were the times where the trauma occurred or even the nightmares. They are now terrified of sleep. Hyper aroused, jacked up nervous system due to all these trauma and nightmares or flashbacks. Helping them get their sleep regulated.
Assisting them get any suicidal or self-harm thoughts under control, aiding them learn not to dissociate so much. Basically a lot of teaching tools that help the person to manage their symptoms, function day to day. Educate them about the impact of the trauma so they don’t feel like they are evil person but help them understand more.
Stage II
If they get stabilised and they want to move on to actually processing the trauma, then start having them talking about and working through their traumas with other trauma focused treatments. Less emphasis on just going over traumas. Pacing has to be done very carefully because they have already been through much. Clinicians need to have training in treating traumatised especially dissociative clients because you don’t want to flood somebody and if that happens they become more symptomatic.
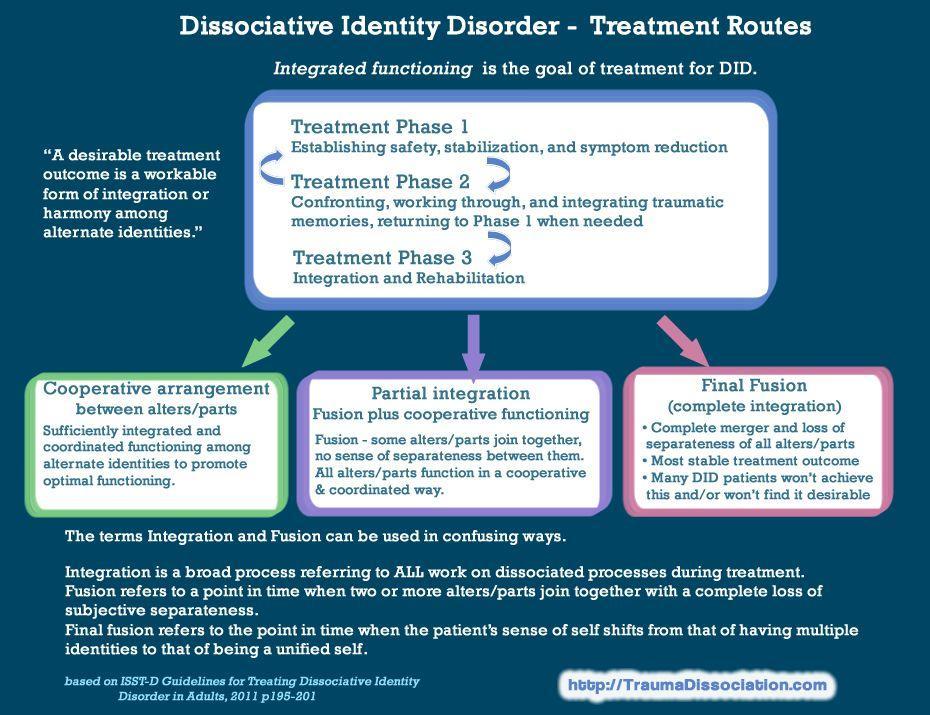
Image source: http://traumadissociation.com/dissociativeidentitydisorder
As they recognize and work though all these traumas there is a ton of grieve that comes along with it. Incredibly painful. When they have DID they have dissociative self-states. So throughout this process they need to get to know their parts gradually and understanding all those parts through them. Shift from the parts fighting with each other (Often when they first come in) to slowly learning to cooperate , collaborate and work more smoothly so that the whole persons functioning is supported and not just one against the other.
Stage III
Less focussed on trauma and focuses on living a full life, having healthy relationships, further establishment of their career.
Are there any specific medication for DID?
- Antidepressants
- Antianxiety drugs to calm them.
- Antipsychotics.
- No specific drug for DID.
Written by Gayathri Gopinadh