
Contents
Overview of Myeloproliferative Disorders
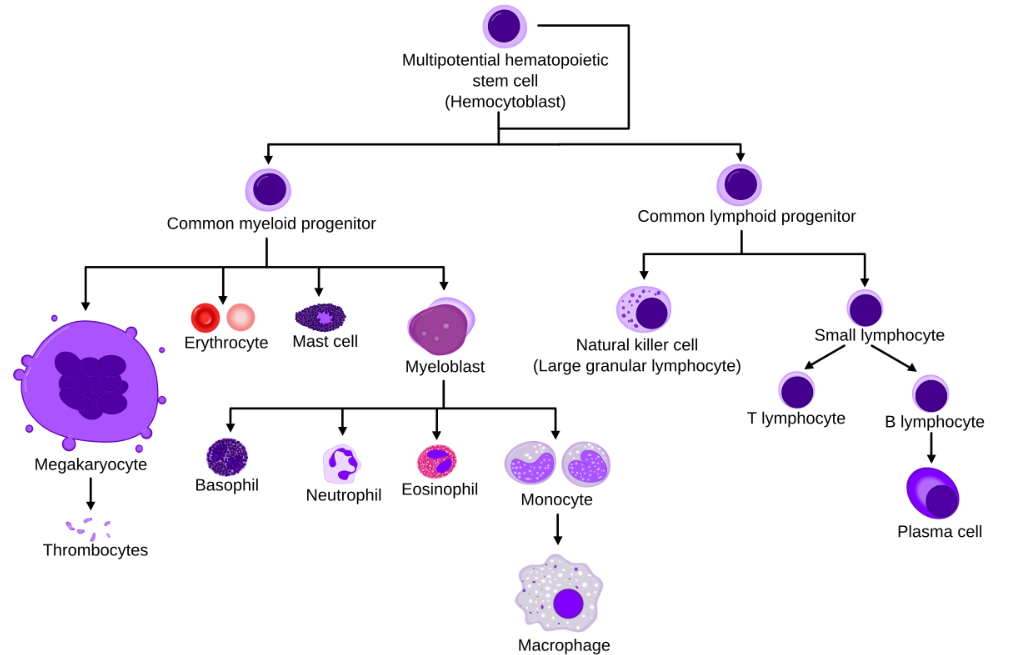
Myeloproliferative disorders generally involve the excessive production of blood cells; specifically, those of the myeloid lineage. The bone marrow produces these cells through a process known as hematopoiesis. The hematopoietic stem cells have the ability to regenerate themselves. These hematopoietic stem cells give rise to the myeloid and lymphoid progenitor cells. Moreover, these cells, further differentiate to ultimately form the different types of blood cells. The conditions inside the bone marrow, like the environment, growth factors, and transcription factors, determine the process of hematopoiesis.
Usually, the myeloid progenitor cells upon differentiation develop into erythrocytes, megakaryocytes, eosinophils, basophils, neutrophils, and monocytes. Similarly, platelets arise from the fragmentation of megakaryocytes. Subsequently, monocytes develop into macrophages and dendritic cells. Subsequently, both of these cells play a major role as phagocytes and antigen-presenting cells to the T cells. Generally, phagocytes are cells that engulf any pathogen or foreign particles and digest them. Subsequently, after digestion, these cells present a fragment of the antigen to the T cells and help in the activation of T cells.
What are myeloproliferative disorders?
If any one of these cells of the myeloid lineage proliferates in an abnormal fashion, then, usually it results in myeloproliferative disorders. Consequently, this can result in various symptoms and complications. Furthermore, these disorders may significantly impact overall health. William Dameshek introduced the words “myeloproliferative disorders” in 1951. The World Health Organisation (WHO) recently changed this term to myeloproliferative neoplasms. The exact cause of myeloproliferative disorders is currently unknown. Usually, myeloproliferative diseases occur in individuals with mutations in the Janus kinase 2 gene. Additionally, people exposed to ionising radiation and toxins are, furthermore, susceptible to this disorder.
Janus kinase 2 gene (JAK2) is the gene responsible for coding proteins that signal the proliferation of the cells. Its proteins send signals to the cell nucleus. This protein controls the production of blood cells from the hematopoietic cells.
Types of myeloproliferative disorders
Chronic myeloid Leukemia
Overview
Chronic myeloid leukemia (CML) belongs to the group of myeloproliferative disorders. Generally, this disease is also referred to as as chronic myelogenous leukaemia or chronic granulocytic leukemia. In general, this disease affects the blood cells and the bone marrow. Usually,this disease affects adults in their middle age, and it is very rare in children. Specifically, this disease affects the granulocytes, and subsequently their number increases. Commonly these cells are usually abnormal as they do not mature properly, and as a result, they do not have the ability to fight against infections. These cells which are not matured properly are called blast.
Causes
The mutation of the genes in the chromosome of the cell causes this disease. A condition called the Philadelphia chromosome occurs in this situation. Specifically, in this condition, a part of the DNA from one chromosome detaches and subsequently attaches to another chromosome. In the case of CML, the ABL part of chromosome 9 exchanges with the BCR gene of chromosome 22. This forms the BCR-ABL fusion gene.
Symptoms
There is no specific symptom for CML. Most of the symptoms are common symptoms; these, along with the diagnostic test can give a conclusive result. The usual symptoms are
- Unusual weight loss
- Feeling very tired
- Soaking night sweating
- Fever
- Pain in the hip region, specifically on the left side.
Diagnosis
Physical examination and health history
A physical examination can give an insight into the patient’s general health, and eventually the doctors can also detect conditions like enlarged spleen. CML patients may experience an increase in spleen size, which can reach up to 5 cm below the left costal edge. The lower part of the thorax is called the costal margin. Costal margin generally refers to the arch formed by the seventh rib to the tenth rib. A health history provides information about the previous diseases and infections the patient has suffered and the treatments they received.
Complete blood count with differential
It is a routine diagnostic process that involves drawing blood from the patient and measuring various blood components, including haemoglobin, platelets, white blood cells (WBC), red blood cells (RBC), and the differential components of WBCs.
Blood biochemistry
Healthcare professionals commonly use this diagnostic procedure to test the elements or components released by the organs and tissues in the blood. This procedure provides insight into any abnormal conditions in the organs or tissues caused by disease or infection.
Bone marrow aspiration and biopsy
In this procedure, a healthcare professional inserts a small needle into the hipbone or breastbone to collect the bone marrow, blood, and a small piece of bone. Subsequently, the team views these samples under a microscope to detect any abnormalities. Some of the tests performed with this sample are
- Cytogenetic analysis
The purpose of this process is to analyse the chromosomes and find any changes in their size, number, brokenness, or excess. The Philadelphia chromosome indicates the presence of cancer. - Fluorescent in situ hybridisation (FISH)
In this test, researchers tag a piece of DNA with a fluorescent dye, which they prepare in a laboratory. This DNA complements specific DNA on the human chromosome. When they mix this fluorescent DNA with the patient’s sample, the tagged DNA pairs with a certain gene in the sample and lights up. This facilitates the identification and counting of DNA. - Reverse transcriptase – polymerase chain reaction (RT-PCR)
This test is helpful in the diagnosis of cancer. This test measures the amount of mRNA (messenger RNA) produced by a certain gene. The enzyme reverse transcriptase converts a specific piece of RNA (ribonucleic acid) into the DNA that generates it. Then, researchers amplify this DNA. Using this amplified DNA, they can identify whether the gene produces a specific mRNA or not.
Treatment
Once a person is diagnosed with CML, it is a general practice to identify the stage or phase of the disease. This phase of the disease is based on the number of blast cells in the blood and the severity of the signs and symptoms of the disease. The diagnosis of the disease’s phase is essential to its therapy. There are 3 stages of CML.
- Chronic: in the chronic phase of CML, less than 10% of the cells in blood and bone marrow are blast cells.
- Accelerated: in the accelerated phase of CML, 10% to 19% of the cells in blood and bone marrow are blast cells.
- Blastic: in the blastic phase of CML, 20% or more of the cells in the blood and bone marrow are blast cells. Generally, it is a blast crisis if the disease is accompanied by tiredness, fever, and enlargement of the spleen during this phase.
- In some cases, CML can recur after a complete cure. This is called relapsed CML.
There are six standard treatment options; they are:
Target therapy
In target therapy, you treat the specific cancer cell with a drug or other substances. In the case of CML, tyrosine kinase inhibition is a form of target therapy. The enzyme tyrosine kinase is blocked in this treatment, which is necessary for stem cell production of white blood cells. In CML, the enzyme is overexpressed, leading to the production of more blast cells. This can be prevented by the treatment. The drugs used are Imatinib mesylate, nilotinib, ponatinib, asciminib, etc.
Immunotherapy
In this type of therapy, the body’s immune cells are used to fight the infection. In the case of CML, interferons are used in immunotherapy, these interferons prevent or slow down tumour growth.
Chemotherapy
Drugs are used in chemotherapy to treat cancer. The drugs are administered parenterally. intravenously, or intramuscularly. The drugs enter the bloodstream and kill the cancer cells.
High-dose chemotherapy with stem cell transplant
Stem cells from the patient or a donor are collected from the bone marrow and frozen. A high dose of antibiotics is used to kill the cancer cells. However, this also results in the body’s stem cells and healthy cells being destroyed. So after chemotherapy, the patient receives an infusion of thawed frozen stem cells that were preserved before.
Donor lymphocyte infusion
This treatment is performed after a stem cell transplant, the lymphocytes from the bloodstream are collected and administered to the patient. These lymphocytes identify the cancer cells as foreign and attack them.
Surgery
Another treatment for CML is the surgical removal of the spleen, also known as splenectomy. This treatment is to relieve the symptoms caused by an enlarged spleen rather than cure the condition.
Polycythemia Vera (PV)
Overview
Polycythemia vera is one of the myeloproliferative disorders. This condition is characterised by an increase in the RBC count. Blood becomes more viscous as a result. This condition also shows a mild increase in the WBC and platelet count.
Causes
This condition is caused by the acquired mutation of the Janus Kinase 2 gene. In this mutation, a valine amino acid is introduced in place of a phenylalanine amino acid at the 617 position of the JAK2 gene, or JAK2V617F. This mutation is characterised by an increase in the cytokine receptors; it is responsible for the increase in the production of RBC and platelets. The mutation is observed in 90%of PV patients. Generally, this mutation is not hereditary. People with PV are at risk of stroke or heart attack caused by blood clots.
Symptoms
The symptoms of PV are due to the increase in the RBC and platelet count which leads to hyperviscosity, thrombosis, and reduced oxygen supply to all the organs. The symptoms include
- Dizziness.
- Ringing of ears.
- Headache.
- Fatigue.
- Vision change.
- Sleeplessness.
- Itchy the whole body, mostly after a hot shower.
- Pain in legs and arms while working or walking.
- Gastritis.
- Feeling full early.
- Nose and gum bleeding.
- Numbness, burning, or tingling on feet and hands.
Diagnosis
Physical examination
A physical examination is done to check for the physical changes that appear during this disease. The physician will check for the enlargement of the spleen, and also check for any redness in the face.
Blood test
A healthcare professional performs a complete blood test, checks the levels of RBC, WBC, and platelets, and reports any abnormal increase in the count of these cells.
Bone marrow test
Blood and tissues are collected from bone marrow for this test. We test the samples to find any genetic abnormalities and observe changes in the count of blood cells.
Genetic analysis
We collect samples from bone marrow for this testing and detect the presence of valine instead of phenylalanine.
EPO levels
Erythropoietin, or EPO, is a hormone that tells bone marrow cells to start making blood cells. PV patients have extremely low EPO levels.
Treatment
There is no cure for the disease. Reducing the intensity of the symptoms is the aim of the treatment. The available treatment includes
- Phlebotomy
In this procedure, blood from patients with PV is removed at regular intervals to maintain the viscosity and cell count of the blood. This process is comparable to blood donation.
- Low dose aspirin
This prevents the platelets from sticking together. This prevents the internal clotting of blood. One disadvantage of this treatment is that the person will be prone to bleeding.
- Medication and chemotherapy
Some medicines, like hydroxyurea, can be used to reduce the count of the blood cells. If this drug causes severe side effects, drugs like busulfan and ruxolitinib can be administered.
Some drugs, like intron A and Besremi, can be used to suppress bone marrow and limit the production of blood cells.
- Surgery
Surgical removal of the spleen is performed to alleviate the symptoms caused by spleen enlargement.
Essential thrombocythemia
Overview
Essential thrombocytopenia (ET) is a condition where the body produces more platelets. One of the myeloproliferative disorders is characterized by an increase in platelet count. In this condition, platelets, formed from megakaryocytes in the bone marrow, are produced in excess. Megakaryocytes fragment to release these platelets into the bloodstream.
Causes
There are three gene mutations responsible for causing ET. They are identified as
- JAK2: Two mutations can occur in this mutation, one mutation occurs in the 617 position of the gene. The phenylalanine residue in this position is replaced with valine. This mutation is expressed as JK2V617F. Another mutation in the JAK2 gene codes for a protein called non-receptor thyrosin kinase; this protein is responsible for the hematopoiesis process.
- CAL: An insertion or a deletion occurs in this mutation, as a result of this a new C terminus is formed. Subsequently, the reading frame is changed. Usually, a protein from this gene is responsible for cellular proliferation, differentiation, and apoptosis.
- MPL: Mutation in this gene is in the form of a point mutation. Usually, this gene codes for thromboprotein receptor protein that is responsible for growth and division of cells, especially the megakaryocytes.
Symptoms
In symptomatic patients, the symptoms include
- Fatigue
- Lack of sleep
- Migraines
- Headaches
- Dizziness
- Various levels of blood clots
- Transient ischemic attacks
- Blood clot in hepatic veins
- Pain and burning in the skin
- Bruise easily
- Mild splenomegaly
Diagnosis
Medical history and physical examination
Medical history gives an insight into the patient’s disease and infection history. We can also find out whether the patient had any blood clotting disorders or hemorrhagic events. A physical examination might be used to detect enlarged spleen or bruising.
Complete blood count with differential
This test measures the number of blood cells. It also detects any deviations in the dimensions and structure of the cells. An increased platelet count of above 450,000/µl can be an indicator for this disease.
Blood clotting
If a patient has a high platelet count, then a blood clotting test has to be performed. An increase in the platelet count can affect the functioning of some of the clotting factors.
Bone marrow test
Blood and bone marrow tissue samples are collected. There will be an increase in the megakaryocytes in the blood from the bone marrow, and they will be abnormal in shape and size.
Genetic analysis
The presence of mutations in the three genes JAK2, CALR, and MPL in the bone marrow tissue is decisive in this disease.
Treatment
The treatment for ET involves the use of low-density heparin to prevent clotting of blood and also medicine that reduces the number of blood cells, like hydroxyurea, anagelide, etc.
Primary myelofibrosis (PMF)
Overview
Myelofibrosis is a condition where scar tissue develops in the bone marrow, and due to the extensive scarring over time, the bone marrow cannot produce healthy blood cells. When myelofibrosis occurs without any triggers, doctors call it primary myelofibrosis. Usually, when other myeloproliferative diseases like PV or ET cause it, doctors refer to it as secondary myelofibrosis.
Causes
The exact cause of the disease remains unknown, but most patients suffering from this disease show the presence of a mutation in JKA2. In about 20% of the patients, doctors observe mutations in the CALR gene.Additionally, 10% of patients have an MPL gene mutation. All of these genes code for proteins that are necessary for signalling the bone marrow to produce blood cells.
Symptoms
Some of the symptoms of PMF are
- Symptoms associated with low RBC: fatigue, shortness of breath, pale skin
- Symptoms due to low WBC count: frequent infection
- Symptoms due to low platelet count: bleeding, bruising
- Symptoms associated with splenomegaly and hepatomegaly: abdominal pain, early satiation, and weight loss.
- Night sweating
- Itching
- Bone and joint pain
- fever
Diagnosis
Physical examination and medical history
During a physical examination, the physical changes caused by the disease are checked. In cases of PMF, paleness of skin, bruises, and enlargement of the spleen can be examined. In medical history, the previous infection and disease suffered by the patients can be evaluated.
Complete blood count test and differential
Blood tests used to determine the quantity of blood cells include differentiation and complete blood count. This test additionally detects abnormalities in the shape and size of the cells.
Bone marrow test
Healthcare professional collects blood and tissues from the bone marrow for bone marrow tests and check for any anomalies.
Genetic analysis
The tissue samples from the bone marrow are analysed for any genetic abnormalities.
- Karyotyping
Usually, the chromosomes are examined using a microscope. Generally, the number and size of chromosomes are studied during this process. They can even identify an extra, missing, deleted, broken, or rearranged chromosome. In some patients with PMF, there can be three or more unrelated chromosomal abnormalities in the chromosomes. This makes it more complex.
- Polymerase chain reaction
The polymerase chain reaction amplifies a small piece of DNA. This process helps scientists study the DNA more easily. This test provides more accuracy and can identify mutations that a microscope cannot detect.
- DNA sequencing
In this procedure, we compare the sequence of the DNA from the patient’s sample with a normal DNA sequence to identify any changes or mutations in it.
Treatment
In asymptomatic patients, usually, no treatment is provided until symptoms appear. Healthcare professionals perform regular checkups to monitor the condition.
In symptomatic patients, treatment involves treating the symptoms. The treatment options are
Stem cell transplant
Healthcare professionals usually perform this procedure on young patients below the age of 60. Usually, the patients receive intensive chemotherapy; after that, subsequently, medical professionals administer stem cells from suitable donors to them in the form of an infusion. Even though this procedure is risky, it is generally in practice as it is the only cure available.
JKA2 inhibitors
JKA2 inhibitors are drugs that block the activity of JKA2 proteins helping in reducing the symptoms of PMF.
A Healthcare professional will perform a splenectomy in patients with severe spleen enlargement to reduce the symptoms.
Reference
- https://www.ncbi.nlm.nih.gov/books/NBK531464/
- https://medlineplus.gov/genetics/gene/jak2/
- https://www.cancer.gov/types/leukemia/patient/cml-treatment-pdq
- https://www.ncbi.nlm.nih.gov/books/NBK531459/
- https://www.webmd.com/cancer/polycythemia-vera
- https://www.hopkinsmedicine.org/health/conditions-and-diseases/polycythemia-vera
- https://www.ncbi.nlm.nih.gov/books/NBK557660/
- https://www.lls.org/myeloproliferative-neoplasms/essential-thrombocythemia
- https://www.ncbi.nlm.nih.gov/books/NBK539709/
- https://www.leukaemia.org.au/blood-cancer/types-of-blood-cancer/myeloproliferative-neoplasms/primary-myelofibrosis/
- https://www.lls.org/myeloproliferative-neoplasms/myelofibrosis/diagnosis
Click here to check Complete Blood Count (CBC) with differential Test
Written by Krishnambal.S
Pingback: Interpretation of results - CBC and Differential counts - HK Technical PGIMS