
Pneumothorax when broken down is 2 words; pneumo meaning air and thorax meaning chest. Abnormal collection or presence of air in the pleural cavity is termed as pneumothorax. The air in the plural space disrupts the normal negative intrapleural pressure which is what is resisting the elastic recoil of the lung tissue keeping them expanded and against the chest wall. Presence of air and pressure decrease the size of the lung and leading to a lung collapse. Collapsed partially or completely.
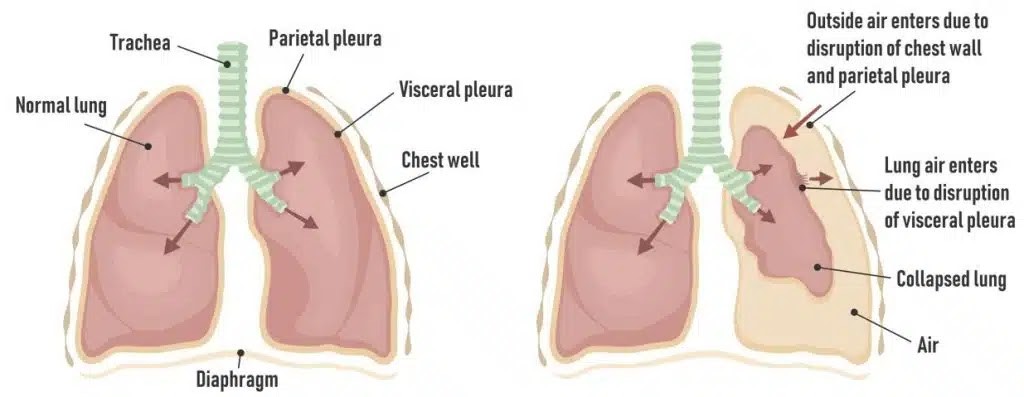
Image source: https://teachmesurgery.com/cardiothoracic-surgery/pleural/pneumothorax/
Symptoms
- Can be asymptomatic in case of primary spontaneous pneumothorax.
- Pleuritic chest pain being the most common one. Sharp, severe or even radiate to the shoulder.
- Dyspnoea
- Asymmetric lung expansion
- Hypoxemia, hypercapnia
- Decreased tactile fremitus
- Tympany on percussion
- Decreased breath sounds
- Impaired respiration and cardiac function (tension pneumothorax)
Primary Spontaneous Pneumothorax
Causes
In this type of pneumothorax there is no known cause. No lung injury or disease. Usually seen in patients who are very tall, thin, young and/or males, EDS (Ehlers Danlos syndrome) or Marfan syndrome.
Pathophysiology
What happens in these patients is that sub pleural apical blebs are formed at the apex. This process just happens in these tall, thin, young and/or males people. Sometimes they can rupture and when it is ruptured they pop. Air can immediately leak from the lung tissue to the pleural space. Air must be there in the lung tissue and within the pleural space.
Secondary Spontaneous Pneumothorax
Causes
Lung injury or underlying lung disease. COPD, asthma, pneumonia, TB, fibrosis, endometriosis, cancer. The patients must have one of the two things. A hyperinflated lungs, which increases the risk of bullae or things like blebs as well. The other one is necrosis of lung tissue. Necrosis could be from infections or malignancies.
Pathophysiology
With hyperinflated lungs, if the lungs are super stretched there is a very high chance that these blebs can pop and air leaking into the pleural space. Especially common in COPD and asthmatic patients. In case of necrosis, if this happens to the lung tissues, there will be rupture and then the air enters into the pleural cavity causing pneumothorax.
Traumatic Pneumothorax
Cause is a trauma, an injury to the lung. Integrity is lost, there is a pleural puncture. Punctured through the parietal pleura, through the visceral pleura, into the lung and then creating a space for air to leak in. External sources will be needles, say while doing thoracentesis, central lines or any other kind of sharp object. It can also occur when large amounts of air are pushed into the lungs of a patient, barotrauma. This is more common in patients under mechanical ventilation.
Complications of Pneumothorax
- The more the air present within the pleural space more is the pressure inside the space.
- Obviously increased pleural pressure can be seen and when this happens it pushes the lungs more likely compressing it.
- The lung compression is in a particular area, say right lower lobe the alveoli in the right lower lobe will be collapsed termed as atelectasis.
- This can lead to V/Q mismatch (ventilation – perfusion mismatch; if the alveolus are squished then there won’t be any space for the air to enter into it and less ventilation which in turn affects the perfusion causing low blood oxygen) and this in turn leads to hypoxemia.
- Patient starts to feel like they are short of breath and will start to breath harder and faster. Respiratory rate will be increased along with the breathing work.
- Respiratory alkalosis and respiratory failure.

Image Source: https://www.geeksforgeeks.org/difference-between-pneumothorax-and-tension-pneumothorax/
Tension Pneumothorax
It can occur due to primary or secondary spontaneous pneumothorax but this is very common with traumatic pneumothorax. During inspiration air enters into the lungs and into the pleural cavity via the space created due to the break between parenchyma and the visceral pleura. During expiration, a one way valve is accidently created which means that on expiration somehow these break within the pleura and the lung parenchyma comes back together. So that the air can’t enter into the lung but stays in the cavity. All the air can come in but none can exit and this will lead to a very high rise in pleural pressure.
All this pressure results in the compression, squeezing of the lung eventually leading to respiratory failure. When the pressure becomes more and more, it presses the lungs and it starts shifting everything to the mediastinum to the opposite side. Trachea will be shifted and it appears to be deviated on examination. Right heart will be compressed impairing the venous return. Reduction in diastolic filling leading to jugular venus distention. Decreased preload due to improper filling of ventricle. Leading to decreased cardiac output and causing hypotension.
Diagnosing it
- Absence of lung markings on chest x ray
- Checking for an underlying lung disease, mechanical ventilation, central lines, recent thoracentesis, history COPD helps in diagnosing.
- Chest CT finding showing bullae or emphysematous findings suggesting secondary pneumothorax.
- Tracheal deviation, mediastinal shift.
Treatment
- Observe the patient if it is not big enough that it will resolve on its own and will not progress to get more worse.
- Oxygen therapy. By doing this there will be created a higher partial pressure of oxygen in the alveoli this is going to create a pressure gradient of nitrogen (most abundant component in the air). This will help to draw the nitrogen out of the pleural space back into the alveoli resolving pneumothorax.
- If it is less than 2 cm from the chest wall to actual pleural line, see if it goes away on its own. Watch them to see any development of serious symptoms leading to respiratory failure.
- Tube thoracostomy on any signs of resp failure or is greater than 2 cm.
- If it develops to tension then needle decompression done.
- Thoracotomy (open or VAT) done in cases where it don’t resolve and have a continuous air leak or trauma.
- Other surgical options done are sewing the blisters, sealing the air leaks, lobectomy
Written by Gayathri Gopinadh